


Program Overview
MCC’s $358 million Lesotho Compact (2008-2013) funded the $144 million Health Sector Project, which aimed to increase access to life-extending anti-retroviral therapy and essential health services by providing a sustainable delivery platform. Among other things, the Project funded the construction or rehabilitation of primary service delivery infrastructure, a National Reference Lab, Blood Transfusion Services, and provided technical assistance and other support related to training, health information systems, and waste management.Evaluator Description
MCC commissioned an independent final performance evaluation of the Lesotho Health Project by Dr. Pim de Graaf. Full report results and learning: https://data.mcc.gov/evaluations/index.php/catalog/217.
Key Findings
Improved Service Delivery Platform
- Crucial health infrastructure was built or rehabilitated and equipped for use, including 138 Health Centers (HCs) and 14 Outpatient Departments (OPDs), though with significant delays and requiring substantial complementary investment from the Government of Lesotho.
- Consensus suggests that the Project provided a necessary platform for health service delivery throughout the country. However, many new HCs lack sufficient space to meet increasing demand, and concerns about the quality of construction and equipment persist.
- National Reference Lab and Blood Transfusion Services have increased their operations, though budgetary and other factors constrain their full service expansion.
Patient and Staff Perceptions
- Patient satisfaction with and use of the facilities has increased, though barriers still exist for pregnant women and people in peripheral communities.
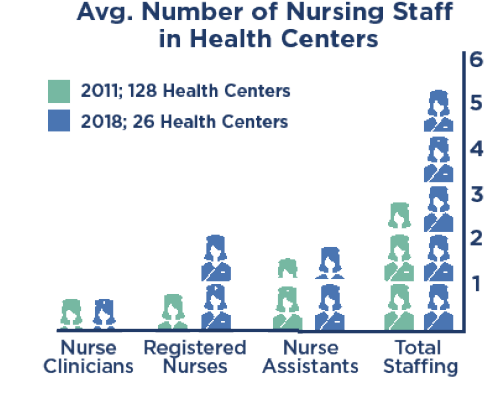
- Staff levels and satisfaction with their living and working conditions have improved. Yet budget constraints keep more than a quarter of sampled health facilities staffed below the current five-nurse staffing complement, especially in hard-to-reach areas.
Progress toward Health Outcomes
- Findings indicate that most population-level health outcomes will require more time to materialize, contrary to MCC’s expectations at the outset, though trends in health care use and improvements in some health-related indicators are encouraging.
Evaluation Questions
This final performance evaluation was designed to answer questions about results from the Project on patients, communities, health professionals, students, and the overall health system. Key evaluation questions include:- 1 Was the program implemented according to plan?
- 2 To what extent have staff perceptions and patients’ perceptions and utilization of HCs and OPDs changed?
- 3 Have overall health outcomes such as infant, child, and maternal mortality, TB treatment success rates, HIV/AIDS treatment, and survival rates changed since the start of the Compact?
Detailed Findings

Improved Service Delivery Platform
The Project constructed and equipped 138 HCs and 14 OPDs but was delayed by more than a year, ran significantly over-budget, and required additional funding from the Government of Lesotho to complete the planned work post-Compact. The dominant perception among stakeholders was that the reconstructed infrastructure, which represents approximately 90% of these facilities in the country, provided a necessary platform for health service delivery throughout the country. However, the new HCs experienced some shortcomings, including design flaws that hindered day-to-day functions; space at the facilities was generally insufficient to accommodate larger patient burdens; and waiting facilities for pregnant women were deficient. In several HCs, tents were being used to alleviate space constraints for special patient groups, including those with HIV/AIDS. Lack of privacy was a major concern. A more localized approach was taken with the reconstruction and equipping of OPDs, where the specific needs of the facility and target population informed their design and implementation.While the National Reference Lab, Blood Transfusion Services, and National Health Training College were all rehabilitated and equipped according to plan, not all of their outputs increased as expected. According to the evaluator, this did not reflect a failure or weakness of the institutions, but rather was a consequence of budgetary constraints that limited staffing and provision of supplies, and in the case of the National Reference Lab, also was a result of decentralization of laboratory functions.
Patient and Staff Perceptions
Patient satisfaction with the health facilities increased significantly from 2011 to 2018, and the new and renovated facilities attract greater use. However, several barriers for accessing care remain, including long distances across difficult terrain, travel expenses, and frequent denial of care if patients arrive later in the day. Pregnant women often still go straight to hospitals or give birth at home due to space constraints, low quality and quantity of meals, or because they lack the infant care items usually required by HCs, e.g., delivery pads and newborn clothing.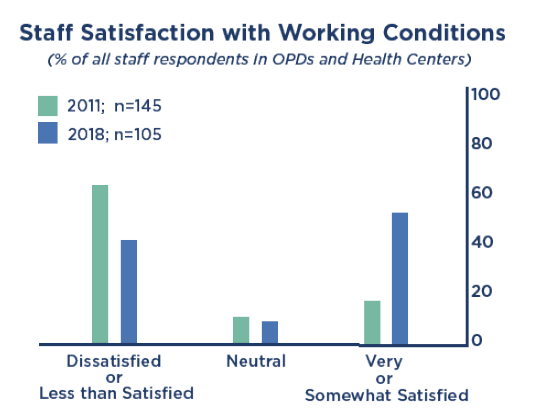
Progress toward Health Outcomes
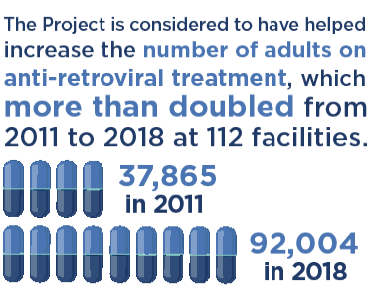
Use of health facilities and related indicators are encouraging. Though the evaluator considers it too early to measure changes in most population-level health outcomes, some of the expected intermediate outcomes have improved. For example, as of early 2017, 98% of people that newly tested positive for HIV in a six-month period were enrolled in an anti-retroviral treatment program, or pre-ARV care. In addition, the number of adults on ARV more than doubled from 37,865 in 2011 to 92,004 in 2018 at 112 facilities supported by the Compact for which data are available. Institutional deliveries of babies increased from 59% in 2009 to 77% in 2014; the number of TB patients receiving care increased; and there have been positive trends in other indicators, such as under-5 mortality and people with HIV still alive 12 months after initial treatment.MCC Learning
- Despite the consensus around the importance of the improved service delivery infrastructure, achieving the ultimate health and productivity aspects of the Project’s objective would likely have required a clearer understanding of the root causes of those problems, and a sharper focus on adequately funding the conditions that are necessary and sufficient to achieve that objective. This lesson has been learned in a number of MCC countries and contexts and MCC has been attempting to address it in more recently-developed compacts.
- Participatory approaches to infrastructure design may take more time, effort, and coordination, but it is important to involve multiple levels of stakeholders to ensure that social infrastructure like health facilities are fit to their purpose. MCC has addressed this lesson by, for example, taking a much more participatory approach to the design of the Morocco II and Cote d’Ivoire schools.
- Compacts need to do maintenance and sustainability planning at the outset, including both how maintenance will be funded and executed, and provide capacity-building to develop an adequate maintenance strategy, if necessary. An explicit sub-Activity was included in the Morocco II Employability Project to develop, test, and begin to rollout a long-term school operations and maintenance policy.
- Reform interventions should target adoption and operationalization rather than just the introduction of policy reform. MCC has been actively exploring how to do effective institutional reform and is currently considering Problem Driven Iterative Adaptation (PDIA) as a strategy in several programs.
- Be cautious when pursuing pipeline randomization designs. Given MCC’s five-year implementation timelines, the time taken to prepare for implementation, and the realities that often occur on the ground, completing one phase of implementation and ensuring a sufficient lag before the beginning of another phase can be very difficult, so should be considered carefully and relevant parties should be committed before investing significant resources in this type of design.
Evaluation Methods

MCC-Funded Health Center in Mafeteng District

Tent Erected at MCC-Funded Outpatient Department in Mafeteng
2019-002-2253